Background of Simethicone Use in Endoscopy
Simethicone, which is comprised of silica gel and dimethicone, is a chemical commonly used as an anti-foaming agent in various medical and industrial applications. In endoscopy, simethicone is used to reduce bubble formation during procedures, while improving visibility of the GI tract. However, its hydrophobic structure and non-polar, covalent attraction introduces significant challenges in terms of effective cleaning and infection control, even when following guidelines.
Letter Templates
Below you will find letters you can download and customize to use at your institution. They contain a wealth of information including scope manufacturers’ guidelines, peer-reviewed studies, the CDC statement, MAUDE data, and other compelling information.
How IP can work with GI
Watch how California APIC President Jessica Alicdan works with her gastrointestinal counterparts in the video below.
How IP can work with GI
Hear tips about simethicone from Mary Ann Drosnock in this video.
Useful Links and Studies
Scope Manufacturers’ Statements on Simethicone Use
Endoscope manufacturers have all recommended against the use of simethicone in conjunction with their scopes. Read the letters below:
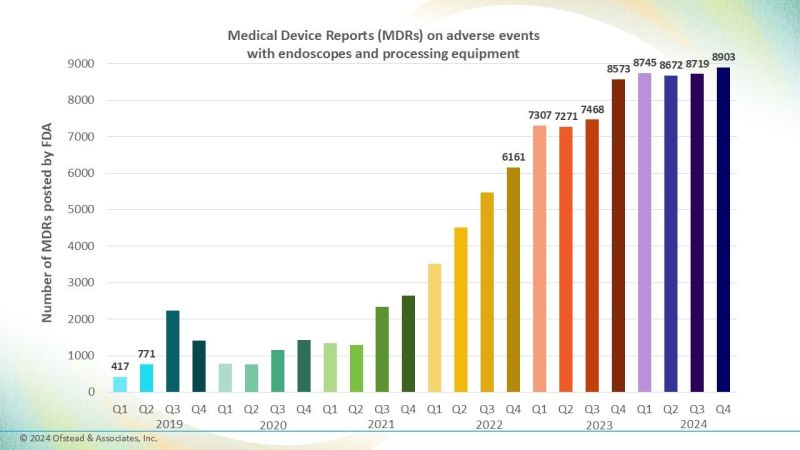
FDA: MAUDE Adverse Events
As the chart below from an Ofstead & Associates LinkedIn post shows, reported infections are growing in the MAUDE database.
Did you know you can search the MAUDE database using this link, and specific year(s) using the search term:
endoscope simethicone
CDC Statement
“Lubricating sprays, simethicone, and other accessories that are not approved for use on these devices may contribute to reprocessing failure.”
Read the entire CDC statement here.
Peer Reviewed Studies
Wang P, et al. Rates of infection after colonoscopy and osophagogastroduodenoscopy in ambulatory surgery centres in the USA. Gut. 2018 Sep;67(9):1626-1636.
According to a landmark study conducted by Johns Hopkins, over 2 million post-endoscopic patients were tracked for 30 days following their procedures. The results revealed a concerning trend—patients who returned to the emergency room with infections were not detected by existing surveillance systems.
The study highlights a significant gap in infection detection and calls for enhanced attention to post-endoscopic care. As physicians, it is crucial to acknowledge that the absence of patient complaints does not equate to the absence of infection.
They found the following 30-day infection rates in their study:
- 1 out of every 250 screening colonoscopies
- 1 out of every 185 non-screening colonoscopies
- 1 out of every 91 EGDs
Barakat MT, et al. Simethicone is retained in endoscopes despite reprocessing: impact of its use on working channel fluid retention and adenosine triphosphate bioluminescence values (with video). Gastrointest Endosc. 2019 Jan;89(1):115-123.
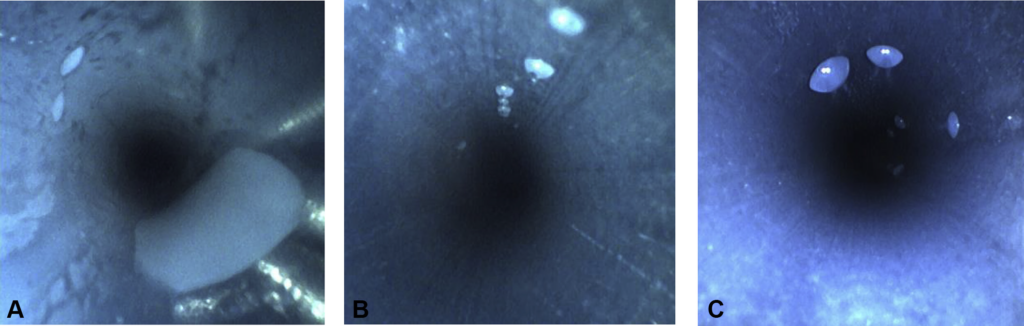
This Stanford study further examined the impact of simethicone, even in diluted forms. Different concentrations of simethicone (3%, 1%, and 0.5%) were administered through the biopsy channels of fully cleaned endoscopes. Despite adhering strictly to cleaning guidelines, including compressed air and a six-hour vertical hanging in a ventilated cabinet, simethicone residues persisted within the working channels.
- Key Findings:
- Even the lowest concentration (0.5%) of simethicone failed to fully clear from the working channels.
- Higher concentrations of simethicone correlated with elevated ATP scores, indicating a greater likelihood of contamination.
This study confirms that no matter how thoroughly scopes are cleaned, simethicone remains a persistent issue, complicating efforts to ensure complete disinfection.
Ofstead CL, et al. Widespread clinical use of simethicone, insoluble lubricants, and tissue glue during endoscopy: A call to action for infection preventionists. Am J Infect Control. 2019 Jun;47(6):666-670.
This study highlights the risks of off-label use of substances like simethicone, lubricants, and tissue glue during endoscopy, which are not fully removed during reprocessing. In four hospitals, microbial contamination was found in over 50% of reprocessed endoscopes, along with residues and fragments indicating incomplete cleaning. These findings suggest that infection preventionists should assess the use of these substances and evaluate reprocessing methods to ensure effective cleaning and reduce infection risks.
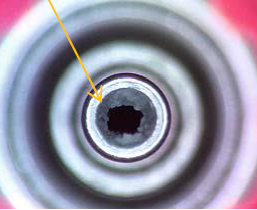
van Stiphout SH, Laros IF, van Wezel RA, Gilissen LP. Crystallization in the waterjet channel in colonoscopes due to simethicone. Endoscopy. 2016 0;48(S 01):E394-E395.
Simethicone’s effects are not limited to infection risk; it can also cause significant damage to endoscopic equipment. In a comprehensive study across 16 facilities, crystallized simethicone was discovered within the water-jets of scopes. This crystallization not only impacts the efficacy of cleaning protocols but also damages Automated Endoscope Reprocessors (AERs) and can migrate between scopes during cleaning cycles. Even bronchoscopes, which do not utilize simethicone, have been affected by cross-contamination.
Additional Resources
Ofstead & Associates – View their full catalog of free webinars on topics related to endoscope reprocessing and quality management, personal protective equipment, biofilm, scientific thinking, and other important sterile processing and infection prevention topics.
Healthmark Academy – an educational platform created by Healthmark, A Getinge company, offering training and resources primarily for healthcare professionals in sterile processing, infection prevention, and medical device reprocessing. Healthmark Academy aims to enhance knowledge, skills, and compliance with industry standards and best practices for staff and patient safety.
The Need for Action
The mounting evidence from multiple studies and real-world data points to one clear conclusion: Simethicone, despite its intended benefits, represents a significant risk in endoscopy.
Infection preventionists and gastroenterologists must take action to mitigate these risks, starting with the removal of simethicone from endoscopic practices. Ensuring that cleaning protocols are both comprehensive and free of agents that contribute to infection persistence is crucial to patient safety.
Contact Us for More Information on Safe Endoscopic Practices
Together, we can improve patient outcomes and ensure the highest levels of care in endoscopic procedures.